In the not-too-distant past, patients seldom, if ever, had an opportunity to meet face-to-face with a radiologist or access their own imaging reports. In addition, providers rarely asked for feedback or considered the patient’s perspective when implementing new policies. But in the age of patient satisfaction, times are changing as radiology practices and hospital radiology departments are implementing patient-centered strategies intended to improve patient care and, in turn, support an increased level of patient satisfaction.
Patient satisfaction is critical given the transition from volume- to value-based care. CMS reimbursements are now tied directly to patient satisfaction scores, especially through the well-known Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) survey. Poor HCAHPS scores cost facilities money, with underperformers losing out on payments. It didn’t take long for providers to make performing well a top priority.
 “The incentive reimbursement based on HCAHPS is far too significant to risk low patient satisfaction scores,” says Eric B. LoMonaco, director of diagnostic and interventional radiology at the Community Hospital of the Monterey Peninsula (CHOMP) in Monterey, Calif. “Private imaging practices also are being paid based on value. Much of that value comes from patient satisfaction, and it is incumbent on providers to implement strategies to make that happen.”
“The incentive reimbursement based on HCAHPS is far too significant to risk low patient satisfaction scores,” says Eric B. LoMonaco, director of diagnostic and interventional radiology at the Community Hospital of the Monterey Peninsula (CHOMP) in Monterey, Calif. “Private imaging practices also are being paid based on value. Much of that value comes from patient satisfaction, and it is incumbent on providers to implement strategies to make that happen.”
So, what have radiologists been doing to “make that happen”? A number of things, it turns out, all in the name of better care, better satisfaction and better reimbursement.
A Building Block
For some imaging practices and radiology departments, adopting a patient communications model built on empathy and a personalized approach ranks among key patient-centered radiology strategies. “This is a building block,” says Mark S. Lerner, RT, division director of radiological operations at George Washington University Hospital in Washington, D.C. “It’s impossible to be at all patient-centered without breaking out of the mold where patients are regarded as ‘the chest x-ray,’ ‘the CT of the liver’ or similar.”
Lerner’s department employs the AIDET healthcare communication framework developed by Studer Group. AIDET stands for “acknowledge,” “introduce,” “duration,” “explanation,” and “thank you.” In accordance with the framework, technologists greet each patient by name, making eye contact and acknowledging any family members or friends in the room. Staff members then introduce themselves and cite their skill set, professional certification and experience, telling the patient the duration of the imaging exam and how much time will elapse before a physician arrives or an update is provided. Next comes a step-by-step explanation of the imaging procedure and what to expect as it occurs, followed by thanking the patient for choosing the facility and thanking the family members or friends for offering their support.
To “signal to patients that they are in a value-based department,” Lerner continues, technologists and other staff utilize an AIDET add-on known as “AIDET Plus-The Promise” when introducing themselves. This involves looking the patient in the eye and saying, “I’m going to take excellent care of you today.”
Taking patients’ individual circumstances into consideration is another iteration of the personalization strategy, according to Jason N. Itri, MD, PhD, assistant professor in the radiology and medical imaging department at the University of Virginia Health System in Charlottesville. Itri explains that his department has configured its technology to prioritize the reading of studies based on such factors as the timing of patients’ appointments with their physicians. For example, if a patient has just undergone an imaging procedure and is scheduled to see his or her physician in two hours, that study would be bumped ahead of others in the queue to accommodate the patient.
“Timely access to reports figures very significantly into patient satisfaction,” Itri says. “No patient is going to be happy if a report isn’t available when it is needed—and being patient-centered in our strategies means making allowances for personal requirements.” A scheduling application that integrates with imaging equipment and reportedly makes it easier to handle requests for imaging appointment changes is currently being tested, Itri adds.
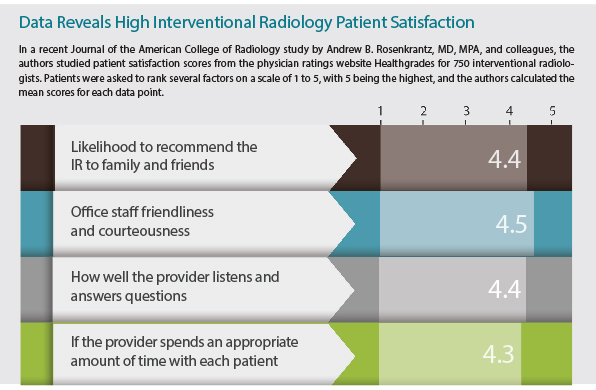
Source: J Am Coll Radiol. 2017 May;14(5):609-614
Upping the Involvement Ante
Strategies aimed at supporting patients’ increased desire to become more invested in their own care are taking hold. This involvement often includes moves by patients to initiate conversations with their physicians, and there has been a move among certain radiology groups and hospitals to facilitate more direct patient/radiologist contact. Jennifer Kemp, MD, a partner in Diversified.
Radiology in Denver, notes that while face-to-face conversations with patients are not always feasible, she and her partners agree to such interaction if requested. Some of Diversified Radiology’s referring physicians bring their patients into the reading room in a wheelchair to review and discuss their images directly with the radiologists.
Kemp says these encounters satisfy patients’ desire to consult with her and her colleagues directly while also giving them an opportunity to hear detailed explanations of study results and have their questions answered in a more complete manner than would otherwise be possible. Moreover, she points out, conversations between radiologists and patients allow the radiologists to calm patients’ fears, encourage them to share specifics about their history that could lead to a more accurate interpretation of the imaging examination, emphasize significant findings and have a thorough, comforting conversation about what happens next.
“A self-serving byproduct of face-to-face interaction is that we radiologists become more visible to patients,” Kemp says. “They learn who we are and learn the value that we bring to the table as part of their physician team.”
Kemp recently introduced a pilot program giving lung cancer screening patients the option to immediately review their scan with a radiologist after it is completed. In addition to paving the way for showing patients their images and discussing findings and recommendations related to lung cancer, she notes, interactions of this type allow her and her colleagues to take patient-centricity to another level by pointing out other findings, such as smoking-induced lung damage. This also gives radiologists a chance to encourage patients to eschew tobacco if they have not already done so. “We can show patients coronary calcifications and discuss potential risks associated with smoking and atherosclerotic disease,” Kemp says. “Lastly, it gives us a chance to explain that lung cancer screening is a yearly test and say that we look forward to seeing them next year for their annual screening.”
Talking frankly is key as is being prepared to go beyond clinical parameters in their conversations, says Ruth C. Carlos, MD, MS, professor of radiology in the division of abdominal radiology for the University of Michigan Health System in Ann Arbor. For example, patients want to discuss quality of life issues when gathering information and making decisions about their treatment. “There are a lot of questions,” she says, “from whether they can ever have a baby and maybe under what conditions, to how much energy they can expect after a course of chemotherapy, to whether it is realistic to plan to buy a house in five years.”
Reading the Report
Providers also have committed time and energy on initiatives to make imaging reports more readily available to patients. At CHOMP, patients have access to their reports through a secure portal 48 hours after the study has been completed. Hospital protocol initially called for immediate report availability, but the waiting period was instituted because referring physicians wanted time to speak with their patients before they view their studies and, potentially, become confused about the findings.
But report accessibility is only part of the equation. In many instances, reports are becoming increasingly patient-centric as they are made more widely available. Under development at CHOMP is a second, patient-facing report, written in lay language and intended to serve as an adjunct to the radiologist’s report. This second report includes details of the imaging procedure, offering an easy-to-understand explanation of what the findings mean and the next steps that need to be taken.
For its part, the University of Virginia Health System is working with a vendor to create reports that will include lay language while also incorporating links to websites that offer pertinent disease-state information. The latter will tie in with the reason for the imaging study.
“Reports and unencumbered access to them often isn’t enough,” says James V. Rawson, MD, radiology department chair at Medical College of Georgia at Augusta University. “Many patients aren’t satisfied unless they can be directed to trusted resources so they can do more research on their own.”
At Augusta University Medical Center, where Rawson works as chairperson of radiology, patient reports include a link to www.RadiologyInfo.org, a website created in a joint endeavor of the Radiological Society of North America and the American College of Radiology. The facility also leverages patient participation in committees and planning initiatives as a strategy for enhancing the quality of care and, in turn, improving patient satisfaction. Three patients presently serve as full members of the hospital’s Quality Steering Committee, which reviews quality metrics and reviews safety issues.
Patient input also is solicited when significant changes are planned that could impact patient care and/or the patient experience. For example, both children and their parents were asked to weigh in when the children’s area of the hospital’s radiology department was slated to undergo a re-design. Based on their feedback, no juvenile-themed artwork was used to decorate the waiting room. Rather, the waiting room features a display of interactive images (an evening cityscape, exploding fireworks and erupting popcorn kernels) that change at 20- to 30-second intervals. To fulfill requests for more child-friendly exam rooms, fixtures in each room can be programmed to emit light in a child’s choice of color. “For us, involving patients of every age in any design process is a major part of the foundation of patient- and family-centered care,” Rawson says.
Communicating in Real Time
Savvy imaging providers have found that patient satisfaction also can be improved by widening communication channels. CHOMP has established a system wherein patients and staff can use their smartphones to scan QR codes posted in the department when a problem or other matter requiring attention arises. Once the code is scanned, an instant message is sent to LoMonaco’s own smartphone so that he may address the situation immediately.
“Empowering patients—and employees, for that matter—to communicate with us in real time has been and continues to be a game-changer when it comes to raising patient satisfaction levels,” LoMonaco says. “It’s easy to turn a situation around while the patient is still at the hospital. Once the person is out the door, it becomes much more difficult.”
The hospital also sends emails to patients prior to their appointments. In addition to a “thank you” for choosing CHOMP for their imaging exams, these communications feature a link patients can click to convey any needs or questions they may have before the appointment. Other specifics provided in those messages include the location of the exam and what the co-pay will be, if there is one.
“Empowering patients to control their own experience is a cornerstone of patient-centric care, and this is just another method of empowerment,” LoMonaco says.
Patient-centered radiology and patient-centered radiology strategies will undoubtedly continue to emerge and evolve as healthcare reform marches on and an increasingly educated, highly engaged base of patients seeks tighter control of their own healthcare destiny. To survive in an era and environment where value is king, private practices and hospitals alike will need to embrace these strategies with open arms.